With Hepatitis C virus (HCV) infection rates four times higher than 10 years ago, patients and clinician rely on a class of anti-viral pills to cure infection and avoid the long-term effects of untreated infection, which include cirrhosis and liver cancer. However, Americans who receive health insurance from Medicaid, which covers over a quarter of all HCV claims in the U.S., could be denied this life-saving medication.
Sam Auty, Paul Shafer, and Kevin Griffith examined Medicaid prescription data to assess how subscription-based payment models (SBPMs) affected access to HCV medications in the Washington state and Louisiana Medicaid programs. SBPMs are an agreement between states and a single manufacturer to supply drugs at a reduced price; they serve as a way to save money on the per person cost of a prescription for HCV treatment. The agreements reached in both the Washington and Louisiana model include a spending cap, so the Medicaid administrators can plan how much money they will spend on HCV medications for the year.
HCV medications are produced by multiple pharmaceutical companies, and the listed prices can be up to $95,000 per prescription in the U.S. A result of these high prices is that most states adopted restrictions limiting which Medicaid enrollees can receive HCV treatment prescriptions. For example, 24 states, including Louisiana prior to the SBPM, had implemented sobriety requirements—persons actively drinking alcohol or using drugs could be excluded.
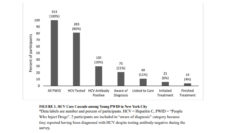
Use of HCV medications increased dramatically, 162.8 per 100,000 Medicaid enrollees, following the subscription agreements.
In preparation for the SBPM implementation, Louisiana Medicaid administrators increased screening efforts and removed their sobriety requirement. Louisiana could lift the restrictions on HCV prescriptions when the SBPM contract took effect because the per person cost would be lower and capped. Individuals previously ineligible due to these restrictions would thus already know their status and be able to receive treatment. Louisiana’s plan for increasing access to HCV medication focused on Medicaid enrollees and incarcerated persons. Use of HCV medications increased dramatically, 162.8 per 100,000 Medicaid enrollees, following the subscription agreements.
Washington did not previously restrict access to treatment, providing prescriptions to all Medicaid enrollees, and their SBPM implementation focused on engagement efforts for screening and treatment for those who inject drugs. Rates of HCV diagnosis and prescriptions did not change significantly; Washington’s numbers may have remained stable because they were already reaching their HCV-infected population prior to their SBPM model took hold, while Louisiana was reaching new communities previously denied access.
SBPMs in several forms allow access to HCV prescription for Medicaid enrollees without putting undue financial burden on states. The subscription-based model’s success demonstrates that agreements to provide affordable medications can greatly improve a state’s liver health if insurance administrators search for and find people at risk.
Photo via Getty Images