Pharmacy Deserts
Twenty-four percent of all LA County census tracts are pharmacy deserts. But they are not created equal.
Read Time: 2 minutes
Published:
Nearly 8% of adults in the United States misuse their prescriptions because their medications are too expensive. Cost is often described as the largest barrier to prescription drug access and adherence, but geography plays a large role as well.
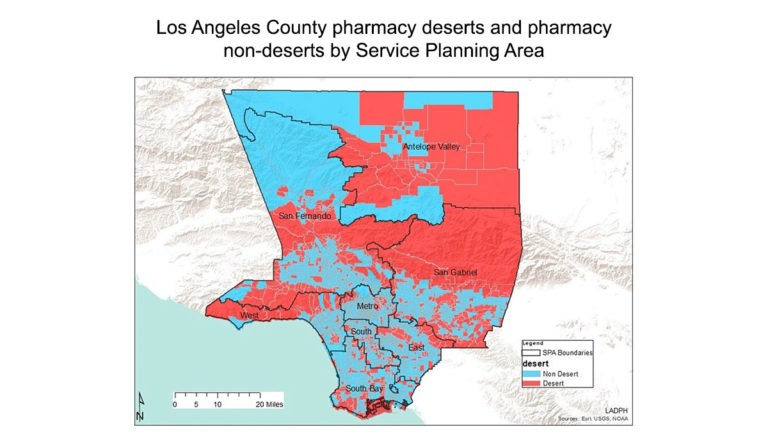
Cheryl Wisseh and team identified distance to the nearest pharmacy as a barrier to care, and defined pharmacy deserts as neighborhoods where the nearest pharmacy is over one mile away. The researchers located every pharmacy in Los Angeles County and analyzed a neighborhood’s distance from the nearest pharmacy alongside racial, ethnic, financial, and other demographics. They mapped their results onto the LA County Department of Public Health’s Service Planning Areas map. In the Figure above, red areas are not within a mile of a pharmacy.
Twenty-four percent of all LA County census tracts are pharmacy deserts. But they are not created equal. Type 1 deserts are homes to more Black and Latinx residents, are more densely populated, and have higher numbers of people living at or below the federal poverty level. Type 2 deserts are whiter, wealthier, and have older populations. People who live in type 2 deserts likely have the means to access pharmacies located farther away.
Improving medication access means recognizing who is in need. This map is an important starting point, although the Angeles National Forest, which has neither residents nor pharmacies, comprises a large portion of the San Gabriel area. While this research helps usher in a new understanding of medication access, a more nuanced map might answer the question: Where should we build the next pharmacy to increase medication access for the largest number of people?
Databyte via Wisseh C, Hildreth K, Marshall J, Tanner A, Bazargan M, Robinson P. Social determinants of pharmacy deserts in Los Angeles County. Journal of Racial and Ethnic Health Disparities. 2020.



