The nearly one million people who seek an abortion in the United States each year face tremendous barriers, including taking time off work, arranging for childcare, traveling long distances to reach a clinic, facing protestors, and paying for the procedure. During the Covid-19 pandemic, many of these barriers have been exacerbated. Medication abortion, which involves taking two drugs, mifepristone and misoprostol, holds promise to increase access. During the pandemic, this method has gained prominence because it can be provided without physical contact.
U.S. Food and Drug Administration regulations prohibit one of the medications, mifepristone, from being distributed through a mail order pharmacy or mailed directly by the clinician. These restrictions have been temporarily relaxed during the pandemic, allowing several virtual abortion clinics to open. Virtual clinics use a direct-to-patient telehealth model of care where patients interact with a healthcare provider by text, video, or phone, provide information about their medical history in lieu of an ultrasound and other screening tests in a clinic, and receive the medications by mail at home. Telehealth abortion care has the potential to reduce out-of-pocket costs for patients, reach those who live far from an abortion provider, and enable people to obtain their care sooner.
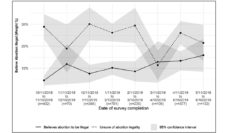
Our research team published findings on the safety and effectiveness of this model of abortion care. We collaborated with a new virtual clinic, Choix, which shared deidentified data from their first 141 patients, served between October 2020 and January 2021. Patients were screened by nurse practitioners using an online form. Some patients were referred to ultrasound to confirm their eligibility but most did not need in-person tests. The service worked with a mail-order pharmacy to mail the medications to eligible patients and followed-up with patients twice to ensure the abortion was complete. We used these data to estimate the number of adverse events patients experienced and any additional medical care they needed to complete the abortion (such as additional medication or an in-clinic aspiration procedure).
We found that 95% of patients had complete abortions without a need for additional medical intervention. None experienced a major adverse event following their abortion. These rates are similar to in-person care, indicating that medication abortion can be provided safely using telehealth, and that the FDA restrictions on medication abortion are not necessary to maintain the current standard of care.
Virtual clinics are one piece of a bigger puzzle of expanding abortion access. Virtual clinics cannot serve patients in the 19 states, including Texas, with laws that effectively prohibit telehealth for abortion. It also remains to be seen whether telehealth can help to address disparities in abortion access by reaching those who face the most barriers, including people of color, low-income people, and those from immigrant communities. We plan to address these questions in our future research.
Telehealth can substantially reduce logistical obstacles to care by allowing patients to complete the entire abortion process from home. Beyond increasing access, direct-to-patient telehealth abortion care can be an empowering model that increases patient convenience, comfort, privacy, and autonomy. It is time for the FDA to permanently remove the burdensome restrictions on mailing mifepristone and for state legislatures to follow the science and allow telehealth for abortion.
Photo via Getty Images