Forty years after the first cases of AIDS were diagnosed in the United States, community-based organizations continue to provide social and clinical support to people living with HIV. But this care was interrupted by Covid-19 as care of the new virus made care of people living with HIV more difficult.
The Boston Health Care for the Homeless Program (BHCHP) suspended in-person services unrelated to Covid-19 during the city’s first pandemic peak (March 16, 2020-May 31, 2020). All non-emergent care was transitioned to telehealth platforms, but with a transiently-housed population, Covid-19 threatened to disrupt the progress in HIV treatment. With financial support from the Ryan White HIV/AIDS Program and the 2020 CARES Act, BHCHP developed an intervention to prevent and respond to Covid-19 among people living with HIV.
The telehealth case management intervention for HIV-positive people experiencing homelessness had two goals. The first was to maintain HIV care during a period of disrupted outpatient services. The second was to reduce Covid-19 transmission by proactively assessing and addressing socioeconomic needs. Dr. Jennifer Brody and colleagues describe this case management initiative in a recent article published in the American Journal of Public Health.
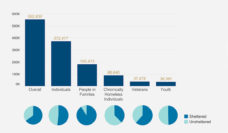
The team started by reviewing electronic health records from the 270 people living with HIV receiving case-management support. Case managers contacted patients with general information about Covid-19 and instructions to access medical testing. Patients without telephones were provided with low-cost cell phones with unlimited minutes. Patients were also contacted bi-weekly to assess their access to personal protective equipment and prescription medication. During those phone calls, BHCHP also assessed food security, transportation needs and status of rental and utility payments. Personal protective equipment was provided by mail to housed patients (defined as those residing in a place with a lease in their name), and during walk-in visits for unhoused patients. Patients in need could also receive grocery gift cards, utility and rental assistance, food delivery and short-term rental or motel vouchers.
By simply providing a reliable method of communication between patients and BHCHP, the organization was better able to assess and respond to needs.
On average, each patient was contacted by phone or in-person by case managers 5.75 times during the three-month study period. Housed patients were contacted 6.43 times whereas unhoused patients received 4.95 contacts. The intervention improved the attendance rate for HIV primary care visits from 63% in the three months before the intervention to 71%.
By simply providing a reliable method of communication between patients and BHCHP, the organization was better able to assess and respond to needs. The reduced barriers to care resulted in patients being more consistent in their primary care visits. This strategy improved the management of HIV and Covid-19 cases by improving accessibility to testing, treatment and medical guidance.
Dr. Brody explained the importance of case management in the following way: “Homeless-experienced people living with HIV have all been made vulnerable — whether by structural racism, poverty, stigma related to addiction, or other forms of overlapping oppression. In order to heal those health harms born of such structural vulnerability, we must continue to push for the integration of structural interventions within biomedical settings.”
This strategy, using telehealth case management and targeted resources to address socioeconomic needs of homeless-experienced people living with HIV, was only feasible with the financial support provided as a response to Covid-19. However, with long-term funding these protocols have the potential to support consistent HIV care as the pandemic winds down.
Photo via Getty Images