Enabling women to plan their families is a bread-and-butter public health issue. South Carolina, like many states, has been working to increase access to contraception, especially long-term contraception like implants and intrauterine devices (IUDs). A simple and technical South Carolina Medicaid innovation in 2012 created a ripple effect that provided birth control to an estimated 100,000 women across the country last year.
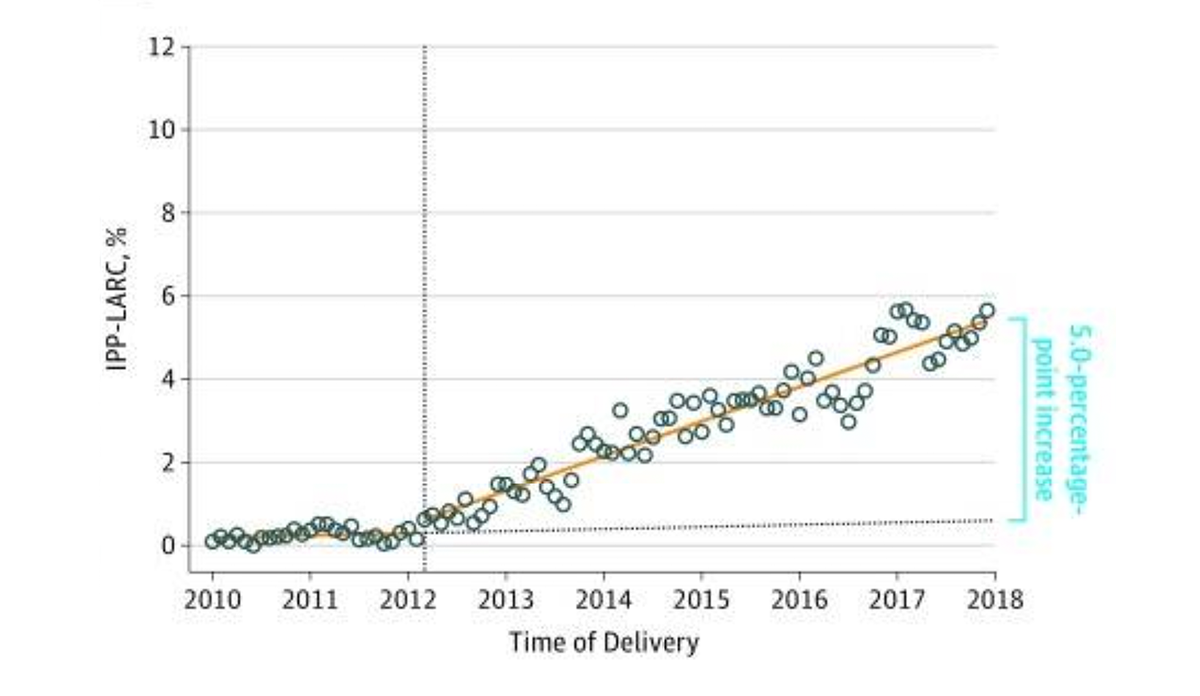
In 2010, just 0.07% of Medicaid beneficiaries who gave birth in South Carolina received a post-delivery IUD or implant. If Medicaid covered this benefit, then why did so few people take advantage of it?
When Medicaid teams investigated, they found that hospitals had no incentive to offer postpartum long-term contraception. When a Medicaid beneficiary is hospitalized for labor and delivery, South Carolina Medicaid provides one standard sum to the hospital for all services provided. So a hospital was paid the same amount whether or not they placed an IUD. Any unused, covered services contributed to the hospital’s profit margin. Hospitals couldn’t deny Medicaid beneficiaries postpartum birth control, but providers didn’t have to offer it. And they didn’t.
In 2012, South Carolina Medicaid began paying for postpartum birth control on top of the lump sum for delivery services. By 2017, 5.7% of adult women and 10.5% of adolescents covered by Medicaid had birth control placed post-delivery.
After the success in South Carolina, 42 other state Medicaid programs and many commercial payers separated reimbursement for postpartum IUDs and implants from the global labor and delivery payment. IUDs and implants are the most effective form of birth control, and creating systems that encourage providers to offer them is a critical step to contraception access.
Databyte via Steenland MW, Pace LE, Sinaiko AD, Cohen JL. Association Between South Carolina Medicaid’s Change in Payment for Immediate Postpartum Long-Acting Reversible Contraception and Birth Intervals. JAMA. 2019;322(1):76-78.