Pregnancy brings birthing people into contact with the health care system when they might not otherwise interact with it. Hence, it represents an opportunity to address both physical and mental health concerns that might never be detected. In a study we published earlier this year we affirmed two key understandings – the importance of simply asking a pregnant or postpartum person if they’re feeling depressed and the persistence of racial disparities.
The impact of postpartum depression on birthing people and their children has led to a number of efforts to better identify those who are at risk for depression, and implement strategies to alleviate symptoms. Notable among these efforts are laws passed in several states requiring screening for depression at postpartum visits. From a political perspective, passing screening requirements is a relatively easy solution. They can be passed as unfunded mandates on providers that allow legislators to take credit for addressing a problem, without incurring the associated costs. We set out to explore postpartum depression with a particular interest in the question, “Does screening matter? “
Our study used data from Listening to Mothers in California, a representative postpartum survey of the experiences of 2,539 Californians who gave birth in 2016. These surveys included a series of questions about clinical screening practices, measured depression and asked if counseling was received.
Several interesting findings emerged. First, postpartum depressive symptoms (detected among 7% of respondents) need to be understood and addressed in the context of chronic depression. We asked respondents if they were experiencing depressive symptoms at the time of the survey and during their pregnancy. Postpartum symptoms of depression, distinct from prenatal symptoms, were relatively rare. Among those respondents reporting prenatal symptoms, 28% reported postpartum symptoms as well. For those reporting no prenatal symptoms, only 3.5% reported new postpartum depressive symptoms.
Health care systems have focused on postpartum depression because of the potentially serious consequences for birthing people and their children. Likewise, we’ve historically only measured depression in the postpartum period. These findings suggest limiting screening to only the postpartum period misses a major opportunity to address a serious chronic illness.
The study also identified who got screened and who got help. Importantly, our question was “…did any maternity care provider ask if you were feeling depressed?” Those saying they were “asked” could be referring to a formal screening or simply a discussion with their provider.
We found rates of postpartum depression were somewhat higher, though not significantly so, among non-LatinX Black respondents compared to LatinX and white respondents. However, rates of being asked about depression were high (79%) and consistent across all race/ethnicity groups. Notably, having symptoms of depression was not correlated with likelihood of screening, suggesting that screening may have more to do with clinical routines than patient mental health status.
Finally, screening is only of value when there is referral to treatment, and effective treatments are available. The United States Preventive Services Task Force, the independent group that reviews all routine screening practices, recognized this need in their screening and intervention recommendations for depressive symptoms in the perinatal period.
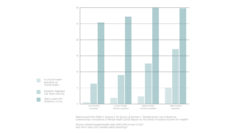
Analysis of who received counseling was noteworthy in two respects. Among birthing people with depressive symptoms, 46% of those who were asked about their mental health got counseling, compared to 20% among those who were not asked. In a multivariable analysis, those asked were almost 6 times more likely to report getting counseling. Secondly, even in the context of high screening rates, racial inequities emerged. Non-LatinX Black respondents with depressive symptoms were only a quarter as likely as non-LatinX Whites to report counseling.
The practical takeaways from this research? From a clinical and policy perspective, the findings suggest both the value of universal screening requirements prenatally as well as postpartum and the continued need to address inequities in service usage by birthing people of color. At a minimum, we need to restructure systems to give providers the opportunity to “Just ask” during visits – especially in the context of universal screening. Equally important, a functional support system must be in place and ready to respond when clinicians identify a problem. with particular attention paid to creating accessible and relevant services for people of color.
NOTE: The article in question is open access and available here.