Public Health Post: How did you develop an interest in precision medicine?
Kirsten Bibbins-Domingo: As a physician who focuses on cardiovascular disease, I am very interested in how preventative efforts reach vulnerable communities. The essence of precision medicine or precision health is using the data and tools available to effectively address health problems. We are living in an era where we have access to more data and an increased ability to understand individual and population health. With faster computational tools, we can really accelerate our understanding of health challenges at hand.
What are the different ways we can understand precision medicine or precision health beyond genomics?
If we look at the original definition, precision medicine is the right therapy to the right person at the right time.
Medicine has always had this goal, but now we have the ability to characterize an individual across multiple domains in real time in the clinical context. We can characterize individuals by their genetics, microbiome, or even the environment in which they live. If I want to think about the health of an individual, it is necessary to think about them across these multiple dimensions.
The traditional blind spot in medicine has been the lack of consideration for the social and environmental factors that influence health. On the other hand, the traditional blind spot in public health has been a lack of acknowledgement of individual heterogeneity that is critical to understanding how best to target interventions.
Precision medicine provides the tools to bridge this gap.
I imagine this type of effort requires a lot of human and technological capability. Do you believe health systems (both medical and non-medical care providers) currently have the capacity to leverage the full potential of what precision medicine could offer?
It is important to point out that we have under-invested in the social sector and over-invested in the medical sector. As a result, there’s a big resource differential—communities with the greatest risk are oftentimes the communities with the fewest resources.
That said, there’s much to be gained from thinking across disciplines and sectors. For instance, health systems are increasing partnerships with public health departments to think about how data can be leveraged across sectors. There is a lot of interest in how public health departments can utilize health system data to inform decisions about public health practice.
For instance, we often have data about hard-to-reach populations like the homeless or those who might have mental illness, but this data sits in a variety of institutions or sectors. If we understand how to connect these data sources, we can identify who within the population needs additional interventions and who might be at-risk. There has been a lot of interest in building this type of capability given the current opioid epidemic.
What are the costs or risks associated with providing precision medicine?
Speaking strictly about the most high-tech form of precision medicine (and arguably, the narrowest), genomic technologies are remarkable underperformers when it comes to usability in the US. This is because most of our genomic data are based on European populations, and the US is far more diverse in reality.
Second, our ability to integrate precision technologies into existing modes of healthcare is fairly limited because frontline providers do not have such technological capabilities within their facilities.
Additionally, while I have talked enthusiastically about integration of social, behavioral, and biological determinants to help develop effective interventions for individuals, there is a real risk of over-medicalizing aspects of social vulnerability.
Are you currently working on a related project that you’re particularly excited about?
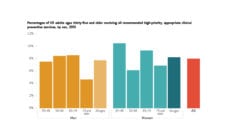
When it comes to primary cardiovascular prevention, we’ve learnt a lot about how to prevent heart disease from traditional epidemiology. We know the factors that put people at risk. We use those factors to understand an individual’s 10-year risk and use our insights to develop targeted interventions. Despite this knowledge, there is still a lack of understanding about effective prevention in young adults because we hardly study young adults.
My work focuses on using precision medicine to better understand the young adult population. I’d love to find the sort of needle in the haystack of the people who are at high risk; people whom I could target my interventions to more specifically.
Photo courtesy of Kirsten Bibbins-Domingo